
Are tiny parasites messing with our brains?
Think before you swallow


Reverie, 1872, Edward Radford (Wikicommons)
Toxoplasma gondii is a tiny protozoan. It’s also a parasite. Like a surprising number of parasites, it can infiltrate brain tissue and make its host behave in ways that help it spread to new hosts.
For example, an infected rat is attracted to the smell of cat urine and ends up getting eaten by a cat, the only host in which T. gondii can sexually reproduce. When the parasite enters a rodent host, through food or water contaminated by cat feces, it targets the amygdala—an area of the brain that stores emotional memories. Autopsies of infected rodents show a density of T. gondii cysts in the amygdala that is twice the density of other brain regions (Vyas et al., 2007). Primates can also get infected, and the behavioral changes are similar. Infected chimpanzees like the smell of leopard urine (Poirotte, 2016).
Although a feline species is the only host in which T. gondii can sexually reproduce, “any warm-blooded predator or omnivore can function as a paratenic host, accumulating different genetically distinct strains of Toxoplasma” (Flegr, 2025). These strains can thus evolve to become more adapted to a new host species, even in the absence of sexual reproduction (Ferguson, 2022).
Humans can get infected—between 13 and 43% of adults 25 to 50 years old in Europe, with lower rates in North America and higher ones in Brazil and Africa (Friesema et al., 2025). Some strains seem to have adapted specifically to human bodies. Of the three main lineages, Type II strains are the most common in our species. They are also much less lethal than Type I, perhaps because they have coevolved with humans to a greater extent (Delgado et al., 2022; Hosseini et al., 2019; Xiao & Yolken, 2015).
Infection causes humans, like other animals, to change mentally and behaviorally. Men become more jealous, women more easy-going, and both sexes slower to respond to threats, as shown by a higher risk of traffic accidents and a longer reaction time. The last finding shows the direction of causality: the longer you have been infected, the slower you react. Slower reaction time does not increase your risk of infection (Flegr et al., 2005; Flegr, 2025; Havlíček et al., 2001; Latifi et al., 2025).
T. gondii manipulates not only behavior but also physical appearance. Infected men are taller, and women rate them as being more dominant and masculine. Infected men also have lower second-to-fourth digit ratios, a sign of greater exposure to the male hormones (Flegr et al., 2005; Flegr, 2025; Hodková et al., 2007; Latifi et al., 2025). This physical manipulation is in line with a strategy of making infected males more attractive to prospective hosts (Mackey & Immerman, 2003).
Can this behavioral and physical manipulation be demonstrated under controlled conditions? Admittedly, we cannot experiment with humans as we do with lab animals. Humans also live long, and decades may pass between the initial infection and the time when the parasite makes its presence known (Cochran et al., 2000; Frost, 2020).
Nonetheless, a group of Czech researchers is convinced that some strains of T. gondii have evolved the ability to manipulate human behavior, specifically sex. Infected men not only seek more sexual partners but also engage in practices that transmit the parasite more efficiently, i.e., into the partner’s oral cavity or anal canal. The male host gets no reproductive benefit; in fact, his fertility is reduced through lower sperm counts and lower sperm motility (Hlaváčová et al., 2021; Kaňková et al., 2020).
At the extremes of sexual behavior, infected individuals, particularly men, feel more drawn to masochism, rape fantasies, bondage, same-sex experiences, and anal sex. Women with latent toxoplasmosis also report feeling more drawn to violent sexual practices and same-sex experiences. But such fantasies are less often acted out by infected individuals. Real changes to sexual behavior seem confined to a greater propensity for sexual promiscuity and oral sex, as well as anal sex among men who have sex with men (Flegr, 2017; Flegr, 2025; Flegr & Kuba, 2016; Latifi et al., 2025).
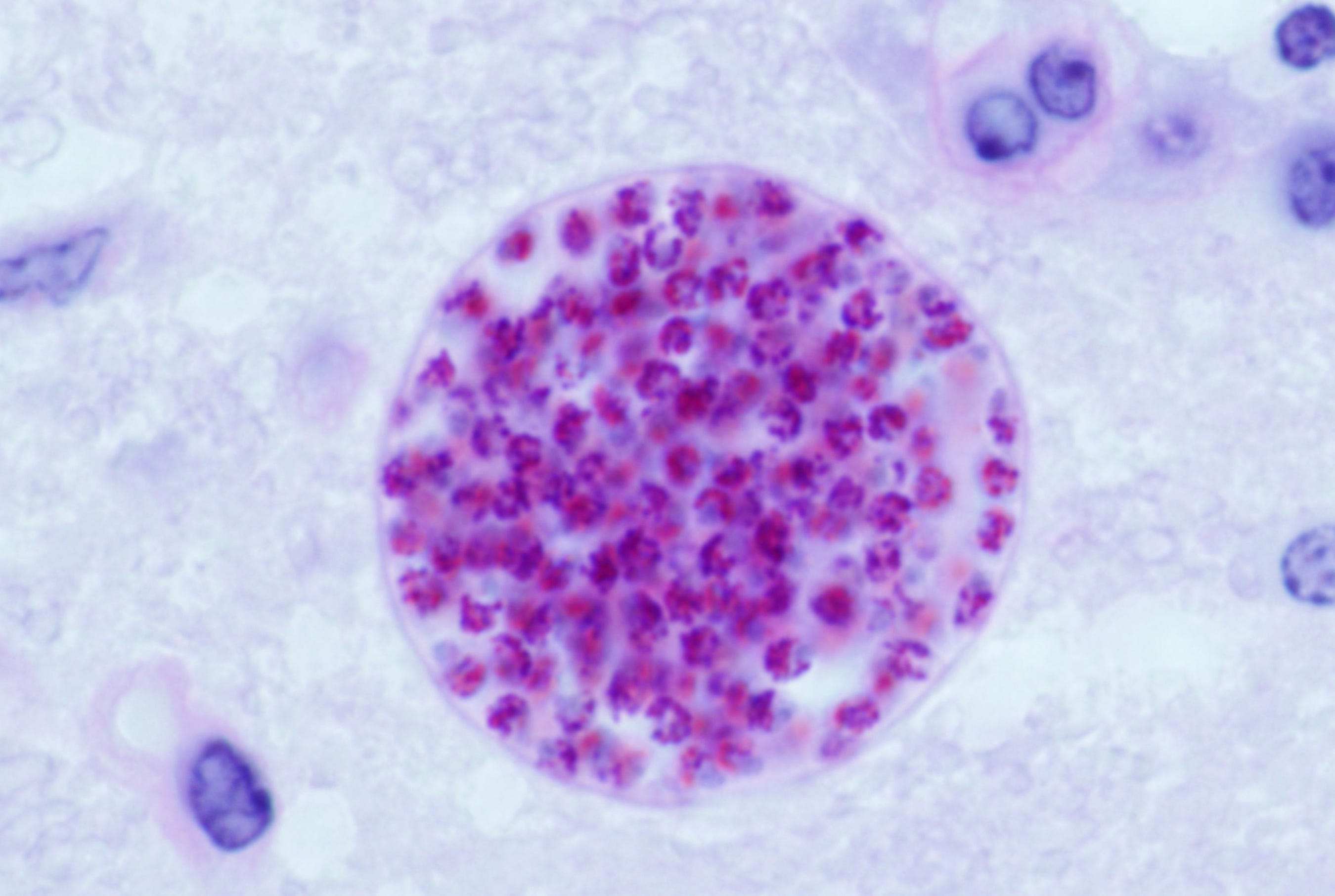
T. gondii cyst in a mouse brain (Wikicommons, J.P. Dubey)
We know that T. gondii is present in semen as cysts containing thousands of spores (Tong et al., 2023). We also know that the cysts are spread from one body to another through fellatio, anal sex, or vaginal sex. The transmission is male to female or male to male, but not female to male (Flegr, 2025; Flegr et al., 2014).
Sexual transmission, particularly from a male host, is indicated by several lines of evidence:
In heterosexual couples, an infected male partner increases the female partner’s risk of infection, but an infected female partner does not increase the male partner’s risk of infection.
In women, the risk of infection correlates with sex work, unprotected sex before pregnancy, and history of genital injuries. In men it correlates with sexual promiscuity, and in male homosexuals with unprotected anal sex.
Seroprevalence of T. gondii is higher in fellating individuals of either sex than in non-fellating controls.
Seroprevalence is higher in homosexuals and promiscuous individuals.
Seroprevalence is positively correlated with the prevalence of STDs across countries, including HIV.
Seroprevalence is higher in women than in men. The gender difference emerges in the 10-to-14 age group and peaks among 20-to-39-year-olds (Flegr et al., 2005; Flegr, 2025; Latifi et al., 2025).
We are only beginning to realize that T. gondii can be sexually transmitted. Most health authorities still believe it is transmitted solely through contaminated food and water or through contact with cats. Yet there must be some sexual transmission, particularly among young men, as shown by the sex ratio of infected individuals. An Italian survey found that recent infections were more frequent in men than in women within the 20 to 40 age bracket (Pinto et al., 2015). A German survey found the rate of seroprevalence to be 1.76 times higher for men, and higher still for younger men (Wilking et al., 2016). An American survey found a rate of 11.25% for males and 9.67% for females (Jones et al., 2017). According to a meta-analysis of workers occupationally exposed to animals, the rate was 63% for male workers and 37% for female workers (Mohammed et al., 2024).
This male predominance, particularly among young adults, seems best explained by a subpopulation of men who have sex with men, either exclusively or occasionally. Alternatively, men in this age bracket are more exposed to cats or contaminated food and water.
T. gondii seems to have gained a capacity for passive sexual transmission and then active sexual transmission through three stages of coevolution with our species:
Entry into a human population, apparently via contact with cats. This animal began to coexist with humans some 10,000 years ago in the Middle East (Galal et al., 2022).
Passive sexual transmission. The parasite was now spreading to other humans via intimate contact but still could not modify human behavior. Natural selection favored those variants that were better adapted to humans. The raw material for evolution did not come from new genetic combinations arising through meiosis during sexual reproduction (which is possible only in a cat’s body). Instead, it came from mutations arising through asexual replication and, less often, through parasexual recombination-like events (Ferguson, 2022).
Active sexual transmission. Natural selection was now favoring those variants that could increase sexual transmission by modifying host behavior.
Sexual transmission of T. gondii remains under-studied due to a research preference for STDs that 1) produce symptoms soon after infection, 2) are easily observable, and 3) develop over a short span of time. These characteristics are not optimal in long-lived species like our own, which can offer an invasive microbe decades of opportunities to infect other individuals. It should therefore remain discreet and do as little harm as possible as long as its host is useful.
Indeed, some diseases of old age may be due not to old age itself but to long-present parasites that have nothing to lose anymore. By that stage of life, the host has stopped having sex, at least on a regular basis, and can be harmed without any real loss. It is only then that the pathogen attracts notice—after a long period of relatively peaceful coexistence. This lengthy coexistence likely involves some degree of behavioral manipulation.
Are other parasites messing with our sex lives?
T. gondii may be one of many microorganisms that have evolved to manipulate human behavior. We are too good to pass up. Our complex neural circuitry, our social nature, and our dense populations make us ideal vectors. Even if a parasite initially has no ability to manipulate human behavior, such an ability could evolve soon enough. All of the right conditions are in place.
The following are several disorders that may be caused by behavior-manipulating microbes. Again, the disorder itself could represent the final destructive stage of a long-term infection.
HIV-Associated Neurocognitive Disorders (HAND)
Although HIV-associated neurocognitive disorders (HAND) are widely attributed to HIV, the relationship between the two remains circumstantial. In fact, HAND occurs even in individuals who have lost all detectable traces of HIV through antiretroviral therapy. Yet 21% of them go on to develop dementia (McArthur & Brew, 2010).
The causal agent seems to be a pathogen other than HIV—an AIDS cofactor, but only in the sense of orienting the host toward behaviors that increase the risk of HIV infection. The pathogen may be hiding in plain sight among the opportunistic infections currently blamed on the host’s compromised immune system. While such infections primarily target the lungs, the brain is the second most-common target (Masliah et al., 2000; Jellinger et al., 2000).
The existence of an HIV cofactor is consistent with the profile of AIDS victims in a study from Bologna, Italy. In that country, AIDS is transmitted mainly via intravenous drug use, yet transmission via homosexuality/bisexuality is ten times more often associated with cognitive impairment (De Ronchi et al., 2002; Wikipedia, 2025). Certainly, AIDS does impair cognition, as shown by an association between low white cell counts and HAND in the Bologna study. But some cofactor must also be impairing cognition via the homosexuality/bisexuality route.
The cofactor might be the hepatitis C virus (HCV). In a large cohort of people with HIV, the risk of HAND was higher among those with antibodies to HCV (Mastrorosa et al., 2023).
Sexually transmissible strains of Candida albicans (vaginal yeast)
This fungal microbe has been implicated in several neurodegenerative diseases, notably Alzheimer's, multiple sclerosis, and autism spectrum disorders (Alonso et al., 2014; Benito-Leon & Laurence, 2017; Hughes & Ashwood, 2018; Pisa et al., 2016). It can thus cross the blood-brain barrier and adhere to tissues in the central nervous system, particularly white matter. Because of antibody cross-reactivity, the actual species is difficult to identify, though C. albicans is the main suspect (Denaro et al., 1995; Jong et al., 2001).
Despite its classification as a single species, C. albicans encompasses many strains that differ substantially in various ways: single nucleotide polymorphisms, inversions, copy number changes, loss of heterozygosity, and whole or partial chromosomal aneuploidies. At least one of these changes is responsible for altering the balance between commensalism and pathogenesis (Hirakawa et al., 2015; see also Tian et al., 2021).
Some strains have adapted specifically to the vagina, with a few causing vulvovaginal candidiasis (VVC). Commonly known as vaginal yeast infection), VVC affects 70 to 75% of sexually active women at least once and 5 to 8% recurrently. In China, two strains account for almost 60% of all VVC cases, with neither being present at extragenital sites (Li et al. 2008).
Sexual transmission is indicated by several lines of evidence:
Once a vaginal infection develops, it can spread to the male partner’s glans penis via vaginal sex or to his oral cavity via cunnilingus (Li et al., 2008; Schmid et al., 1995).
The same strains seem to infect both the vagina and the glans penis (Ge et al., 2012; see also Tian et al., 2021).
In both men and women, genital yeast infections are associated with a higher number of sexual partners (Warszawski et al., 1996).
There seems to have been selection for sexual transmissibility, particularly via oral sex. Vaginal strains adhere better than other strains to saliva-coated surfaces (Schmid et al. 1995).
Transmission is female to male and not male to female. Infected people do not have higher rates of vaginal sex but do have higher rates of oral sex, notably cunnilingus (Hellberg et al., 1995; Reed et al., 2003). C. albicans in the male partner’s oral cavity does not predict recurrence of VVC in the female partner (Reed et al., 2003), and treatment of the male partner with antifungals does not prevent recurrence of VVC in the female partner (Bisschop et al., 1986; Buch et al. 1982).
Infection goes through three stages: 1) colonization of the vagina as a commensal with low virulence and no VVC, potentially for a long period of relative latency; 2) colonization of brain sites that influence sexual behavior; and 3) activation of the VVC stage, during which the pathogen can spread to a male partner. The final stage is when the parasite may alter the behavior of its female host, perhaps by weakening her sexual inhibitions and encouraging vaginal contact with her partner’s body, particularly his mouth.
Multiple sclerosis
This disease can cause lesions throughout the nervous system, often the limbic system of the brain and particularly the amygdala (Batista et al., 2016; Hillyer et al., 2023; Meyer-Arndt et al., 2022). As we have seen with T. gondii, this brain region is a primary target for manipulation of behavior.
Multiple sclerosis (MS) seems to be associated with a fungal parasite that infiltrates the brain and nervous system, perhaps a form of Candida. In people with MS, this association is indicated by:
Antibodies against various Candida species
High levels of immune defense proteins that bind to mannoproteins, which are ubiquitous in fungal cell walls but rare in bacterial and mammalian cell walls
High levels of chitotriosidase, which the immune system produces to destroy chitin—a component of fungal cell walls but not of bacterial and mammalian cell walls.
Successful treatment of MS with a fungicide, dimethyl fumarate (Benito-Leon & Laurence, 2017).
MS seems to be sexually transmitted. It is rare before puberty, two to three times more common in women, more common in women taking oral contraceptives, and associated with smoking—a sociological marker of sexual activity among women. It is also associated with herpes simplex virus type 2 (Benito-Leon & Laurence, 2017; Golden & Voskuhl, 2017; Hawkes, 2002).
Unlike the unknown parasite that causes HAND, the one that causes MS begins doing harm early in adulthood, at around 30 years of age, perhaps because this is when female hosts tend to abandon their multi-partner lifestyle. Consequently, the parasite no longer has anything to gain from keeping its host healthy. The mean age of onset for MS has nonetheless risen in recent decades (Golden & Voskuhl, 2017; Romero-Pinel et al., 2022).
A role in alternative sexualities?
We will now turn to alternative sexual lifestyles. Could these also be due, in some cases, to behavioral manipulation by unknown parasites?
The caveat “in some cases” should be highlighted, since such parasites must become sexually transmissible before they can evolve the ability to manipulate sexual behavior. They should thus facilitate an existing behavior, which would exist even without them. Nonetheless, as we shall see, creation of novel behaviors is not excluded.
Exclusive male homosexuality
More than two decades ago, Greg Cochran argued for the existence of a “gay germ,” i.e., a pathogen that reorients male sexual preferences to increase the number of hosts it can infect via sexual relations (Cochran et al., 2000). He ruled out a genetic cause because of the high fitness cost of exclusive male homosexuality and its heritability of only 20%. Instead, the cause may be a pathogen that targets the limbic system. “Indeed, anecdotal reports indicate that changes in human sexual orientation have occurred following changes in the limbic area due to trauma or infection.” The pathogen may be exploiting a niche that provides more opportunities for sexual transmission. “[H]omosexual behavior could facilitate spread because of the larger numbers of partners homosexual males may have on average, relative to heterosexual males” (Cochran et al., 2000).
This theory may be supported by recent findings about the gut microbiome of men who have sex with men. Specifically, they have fewer of the commensal bacteria that help repair and preserve the intestinal lining. Perhaps an invasive pathogen destroys such bacteria in order to facilitate its entry into the body. Although the altered microbiome facilitates HIV infection, having been in fact discovered through AIDS research, HIV itself does not seem to be responsible (Armstrong et al., 2018; Lin et al., 2024; Tuddenham et al., 2020).
Cuckold fetish
Other pathogens may cause certain paraphilias, such as the cuckold fetish—where a man no longer feels sexual jealousy and even derives pleasure from the prospect of being cuckolded. This fetish is not mentioned in Greco-Roman literature, which nonetheless attests to a wide range of alternative sexualities. The earliest references come from 17th century England, where it was said to be common among merchants (Frost, 2023).
The date and milieu point to an external source—most likely, slaves imported through trade from West Africa. The region’s high polygyny rate would have been conducive to the evolution of STDs that can spread from one polygynous household to another. Keep in mind that the barriers to transmission were already low. On the one hand, the head of household was generally an older man who could not satisfy all his wives; on the other, the latter were often solicited by young single men, as inevitably happens in a polygynous society.
This point is made by anthropologist Pierre van den Berghe:
The temporary celibacy of young men in polygynous societies is rarely absolute, however. While it often postpones the establishment of a stable pair-bond and the procreation of children, it often does not preclude dalliance with unmarried girls, adultery with younger wives of older men, or the rape or seduction of women conquered in warfare. Thus, what sometimes looks like temporary celibacy is, in fact, temporary promiscuity. (van den Berghe, 1979, pp. 50-51)
Polygynous households were thus vulnerable to any STD that could overcome the already low barriers to entry. Once this behavioral niche was colonized, selection favored those strains that could further lower the barriers by inhibiting or even reversing male jealousy.
Conclusion
In theory, all STD pathogens should be under selection for the ability to manipulate host behavior. Their very existence depends on how the host behaves, and even a slight behavioral change could significantly improve their ability to infect other individuals. Sexual transmission is an ideal target for manipulation because it provides the pathogen with potentially numerous opportunities for spreading to new hosts.
Such manipulation can take different forms. Some pathogens may make the male or female host less discriminating, as is the case with T. gondii. Others may reorient the host’s sexual orientation. Still others may cause sexual fetishes and other paraphilias. In fact, all STDs may be evolving to some degree along this trajectory. It has been suggested that certain well-known ones (HIV, HPV, Chlamydia trachomatis, Neisseria gonorrhoeae) help an infected individual continue to infect others by suppressing production of pro-inflammatory cytokines and thereby inhibiting the loss of interest in sex that comes with sickness behavior (Adamo, 2014).
It is difficult to determine the full extent of this phenomenon. One avenue of research would be to examine the human brain for signs of strategies to counter behavioral manipulation, as two evolutionary biologists have wondered:
How much of our neural complexity is a necessary defense against manipulative invaders? How much of the enormous redundancy is to provide system level functionality if part of the system is attacked? How much of the complex process of wiring a brain during development is to prevent pathogen re-wiring? (Read & Braithwaite, 2012, p. 195)
These defensive strategies achieve their aim in three ways: 1) restrict access to the brain, primarily by defending the blood-brain barrier; 2) increase the costs of manipulation, either by increasing the amount of neuroactive substance needed for a behavioral response or by making this substance toxic at the microscopic level; and 3) increase robustness, by creating redundant or modular neural systems as “backups” to ensure the integrity of behavioral responses (Del Giudice, 2019).
The first strategy may be attested by the presence of decoy surface molecules. Such decoys mimic the surface molecules used by invasive pathogens to enter a cell while not allowing them to enter. An example in humans is CEACAM3, which mimics the normal surface molecule CEACAM1. It is fast-evolving in our species, apparently because it has been in an evolutionary arms race with certain pathogens: the latter evolve to avoid this surface molecule, which in turn evolves to bind the pathogen even more (Del Giudice, 2019). Are such decoys produced by our neural tissues?
Evolutionary psychologist Marco Del Giudice is skeptical about the possibility that behavior-manipulating parasites have adapted to human bodies, notably because of the size and complexity of our brains. We thus have so much neural redundancy that a parasite would have to pull too many switches in too many places to produce a substantial effect. We are also much bigger than any invasive microbe and can metabolically invest much more in counter-measures.
Other things, however, do not work in our favor. First, we have a much longer generation time than any invasive microbe. The latter can evolve faster than we can. Second, while our large, complex brains are more difficult to control completely, they offer more opportunities for partial control. Third, as already noted, if the parasite is sufficiently discreet, at least until its human host is too old to have sex, the cost of its presence may be too low for the host to invest in rigorous countermeasures.
But one other thing does work in our favor: humans can fight parasites through cultural rules and prohibitions. Rules against sexual promiscuity and non-vaginal sex may reflect a vague awareness that the sex act can transmit not only semen but also unwanted free riders (Mackey & Immerman, 2001; Mackey & Immerman, 2003).
References
Adamo, S. A. (2014). Parasitic aphrodisiacs: manipulation of the hosts’ behavioral defenses by sexually transmitted parasites. Integrative and Comparative Biology, 54(2), 159-165. https://doi.org/10.1093/icb/icu036
Alonso, R., Pisa, D., Rábano, A., & Carrasco, L. (2014). Alzheimer’s disease and disseminated mycoses. European Journal of Clinical Microbiology & Infectious Diseases, 33(7), 1125-1132. https://doi.org/10.1007/s10096-013-2045-z
Armstrong, A. J., Shaffer, M., Nusbacher, N. M., Griesmer, C., Fiorillo, S., Schneider, J. M., ... & Lozupone, C. A. (2018). An exploration of Prevotella-rich microbiomes in HIV and men who have sex with men. Microbiome, 6(1), 198. https://doi.org/10.1186/s40168-018-0580-7
Batista, S., d’Almeida, O. C., Afonso, A., Freitas, S., Macário, C., Sousa, L., ... & Cunha, L. (2017). Impairment of social cognition in multiple sclerosis: Amygdala atrophy is the main predictor. Multiple Sclerosis Journal, 23(10), 1358-1366. https://doi.org/10.1177/1352458516680750
Benito-Leon, J., & Laurence, M. (2017). The Role of Fungi in the Etiology of Multiple Sclerosis, Frontiers in Neurology 16 October https://doi.org/10.3389/fneur.2017.00535
Bisschop, M. P. J. M., Merkus, J. M. W. M., Scheygrond, H., & Van Cutsem, J. (1986). Co‐treatment of the male partner in vaginal candidosis: a double‐blind randomized control study. BJOG: An International Journal of Obstetrics & Gynaecology, 93(1), 79-81. https://doi.org/10.1111/j.1471-0528.1986.tb07818.x
Buch, A., & Christensen, E. S. (1982). Treatment of vaginal candidosis with natamycin and effect of treating the partner at the same time. Acta Obstetricia et Gynecologica Scandinavica, 61(5), 393-396. https://doi.org/10.3109/00016348209156578
Cochran, G.M., Ewald, P.W., & Cochran, K.D. (2000). Infectious Causation of Disease: An Evolutionary Perspective. Perspectives in Biology and Medicine, 43(3), 406-448. https://doi.org/10.1353/pbm.2000.0016
De Ronchi, D., Faranca, I., Berardi, D., Scudellari, P., Borderi, M., Manfredi, R., & Fratiglioni, L. (2002). Risk Factors for Cognitive Impairment in HIV-1-Infected Persons with Different Risk Behaviors. Archives of Neurology, 59(5), 812-818. https://doi.org/10.1001/archneur.59.5.812
Delgado, I. L., Zúquete, S., Santos, D., Basto, A. P., Leitão, A., & Nolasco, S. (2022). The apicomplexan parasite Toxoplasma gondii. Encyclopedia, 2(1), 189-211. https://doi.org/10.3390/encyclopedia2010012
Del Giudice, M. (2019). Invisible designers: brain evolution through the lens of parasite manipulation. The Quarterly Review of Biology, 94(3), 249-282. https://doi.org/10.1086/705038
Denaro, F.J., López-Ribot, J.L., & Chaffin, W.L. (1995). Adhesion of Candida albicans to Brain Tissue of Macaca mulata in an Ex Vivo Assay. Infection and Immunity , 63(9), 3438-3441. https://doi.org/10.1128/iai.63.9.3438-3441.1995
Ferguson, D.J.P. (2022). Toxoplasma gondii: Detailed Description of the Coccidian (Asexual and Sexual) Development and Oocyst Sporulation. In: de Souza, W. (eds) Lifecycles of Pathogenic Protists in Humans. Microbiology Monographs, vol 35. Springer, Cham. https://doi.org/10.1007/978-3-030-80682-8_9
Flegr J. (2013). Influence of latent Toxoplasma infection on human personality, physiology and morphology: pros and cons of the Toxoplasma-human model in studying the manipulation hypothesis. Journal of Experimental Biology, 216, 127–133. https://doi.org/10.1242/jeb.073635
Flegr, J. (2017). Does Toxoplasma infection increase sexual masochism and submissiveness? Yes and no. Communicative & integrative biology, 10(5-6), e1303590. https://doi.org/10.1080/19420889.2017.1303590
Flegr, J. (2025). Thirty years of studying latent toxoplasmosis: behavioural, physiological, and health insights. Folia Parasitologica, 72, 1-16. http://dx.doi.org/10.14411/fp.2025.005
Flegr, J., Hrŭsková, M., Hodný, Z., Novotná, M., & Hanušová, J. (2005). Body height, body mass index, waist-hip ratio, fluctuating asymmetry and second to fourth digit ratio in subjects with latent toxoplasmosis. Parasitology, 130(6), 621-628. https://doi.org/10.1017/S0031182005007316
Flegr, J., Klapilová, K., & Kaňková, Š. (2014). Toxoplasmosis can be a sexually transmitted infection with serious clinical consequences. Not all routes of infection are created equal. Medical Hypotheses, 83(3), 286-289. https://doi.org/10.1016/j.mehy.2014.05.019
Flegr, J., & Kuba, R. (2016). The relation of Toxoplasma infection and sexual attraction to fear, danger, pain, and submissiveness. Evolutionary Psychology, 14(3), 1474704916659746. https://doi.org/10.1177/1474704916659746
Friesema, I. H., Waap, H., Swart, A., Györke, A., Le Roux, D., Evangelista, F. M., ... & Opsteegh, M. (2025). Systematic review and modelling of Toxoplasma gondii seroprevalence in humans, Europe, 2000 to 2021. Eurosurveillance, 30(34), 2500069. https://doi.org/10.2807/1560-7917.es.2025.30.34.2500069
Frost, P. (2023). Cuckoldry: Sexual Fantasies. In: Shackelford, T.K. (ed.) Encyclopedia of Sexual Psychology and Behavior. Springer. https://doi.org/10.1007/978-3-031-08956-5_757-1
Frost, P. (2020). Are Fungal Pathogens Manipulating Human Behavior? Perspectives in Biology and Medicine, 63(4), 591-601. https://doi.org/10.1353/pbm.2020.0059
Galal, L., Ariey, F., Gouilh, M. A., Dardé, M. L., Hamidović, A., Letourneur, F., ... & Mercier, A. (2022). A unique Toxoplasma gondii haplotype accompanied the global expansion of cats. Nature Communications, 13(1), 5778. https://doi.org/10.1038/s41467-022-33556-7
Ge, S. H., Xie, J., Xu, J., Li, J., Li, D. M., Zong, L. L., ... & Bai, F. Y. (2012). Prevalence of specific and phylogenetically closely related genotypes in the population of Candida albicans associated with genital candidiasis in China. Fungal Genetics and Biology, 49(1), 86-93. https://doi.org/10.1016/j.fgb.2011.10.006
Golden, L.C., & Voskuhl, R. (2017). The Importance of Studying Sex Differences in Disease: The example of Multiple Sclerosis. Journal of Neuroscience Research, 95(1-2), 633-643. https://doi.org/10.1002/jnr.23955
Havlíček, J., Gasová, Z. G., Smith, A. P., Zvára, K. & Flegr, J. (2001). Decrease of psychomotor performance in subjects with latent ‘asymptomatic’ toxoplasmosis. Parasitology, 122, 515-520. https://doi.org/10.1017/S0031182001007624
Hawkes, C. H. (2002). Is multiple sclerosis a sexually transmitted infection?. Journal of Neurology, Neurosurgery & Psychiatry, 73(4), 439-443. https://doi.org/10.1136/jnnp.73.4.439
Hellberg, D., Zdolsek, B., Nilsson, S., & Mårdh, P. A. (1995). Sexual behavior of women with repeated episodes of vulvovaginal candidiasis. European Journal of Epidemiology, 11, 575-579. https://doi.org/10.1007/BF01719311
Hillyer, A., Sharma, M., Kuurstra, A., Rosehart, H., Menon, R., & Morrow, S. A. (2023). Association between limbic system lesions and anxiety in persons with multiple sclerosis. Multiple Sclerosis and Related Disorders, 79, 105021. https://doi.org/10.1016/j.msard.2023.105021
Hirakawa, M. P., Martinez, D. A., Sakthikumar, S., Anderson, M. Z., Berlin, A., Gujja, S., ... & Cuomo, C. A. (2015). Genetic and phenotypic intra-species variation in Candida albicans. Genome research, 25(3), 413-425. http://www.genome.org/cgi/doi/10.1101/gr.174623.114
Hlaváčová J., Flegr J., Řežábek K., Calda P., Kaňková Š. (2021). Association between latent toxoplasmosis and fertility parameters of men. Andrology, 9, 854–862. https://doi.org/10.1111/andr.12969
Hodková H., Kolbeková P., Skallová A., Lindová J., & Flegr J. (2007). Higher perceived dominance in Toxoplasma infected men – a new evidence for role of increased level of testosterone in toxoplasmosis-associated changes in human behaviour. Neuroendocrinology Letters, 28, 110–114.
Hosseini, S.A., Amouei, A., Sharif, M., et al. (2019). Human toxoplasmosis: a systematic review for genetic diversity of Toxoplasma gondii in clinical samples. Epidemiology and Infection, 147:e36. https://doi.org/10.1017/S0950268818002947
Hughes, H.K., & Ashwood, P. (2018). “Anti-Candida albicans IgG Antibodies in Children with Autism Spectrum Disorders.” Frontiers in Psychiatry, 9, 627. https://doi.org/10.3389/fpsyt.2018.00627
Jellinger, K.A., Setinek, U., Drlicek, M., Böhm, G., Steurer, A., & Lintner, F. (2000). Neuropathology and General Autopsy Findings in AIDS during the Last 15 Years. Acta Neuropathologica, 100(2), 213-220. https://doi.org/10.1007/s004010000245
Jones, J. L., Kruszon-Moran, D., Elder, S., Rivera, H. N., Press, C., Montoya, J. G., & McQuillan, G. M. (2017). Toxoplasma gondii infection in the United States, 2011–2014. The American Journal of Tropical Medicine and Hygiene, 98(2), 551. https://doi.org/10.4269/ajtmh.17-0677
Jong, A.Y., Stins, M.F., Huang, S-H., Chen, S.H.M., & Kim, K.S. (2001). Traversal of Candida albicans across Human Blood-Brain Barrier In Vitro. Infection and Immunity, 69(7), 4536-4544. https://doi.org/10.1128/iai.69.7.4536-4544.2001
Kaňková Š., Hlaváčová J., Flegr J. (2020). Oral sex: a new, and possibly the most dangerous, route of toxoplasmosis transmission. Medical Hypotheses, 141, 109725. https://doi.org/10.1016/j.mehy.2020.109725
Kurtzke, J. F., Hyllested, K., Heltberg, A., & Olsen, A. (1993). Multiple sclerosis in the Faroe Islands. 5. The occurrence of the fourth epidemic as validation of transmission. Acta neurologica scandinavica, 88(3), 161-173.
Latifi, A., Flegr, J., & Kaňková, Š. (2025). Re-assessing host manipulation in Toxoplasma: the underexplored role of sexual transmission–evidence, mechanisms, implications. Folia Parasitologica, 72, 015. http://dx.doi.org/10.14411/fp.2025.015
Li, J., Fan, S. R., Liu, X. P., Li, D. M., Nie, Z. H., Li, F., ... & Bai, F. Y. (2008). Biased genotype distributions of Candida albicans strains associated with vulvovaginal candidosis and candidal balanoposthitis in China. Clinical Infectious Diseases, 47(9), 1119-1125. https://doi.org/10.1086/592249
Lin, H., Chen, Y., Abror-Lacks, G. et al. (2024). Sexual behavior is linked to
changes in gut microbiome and systemic inflammation that lead to HIV-1
infection in men who have sex with men. Communications Biology, 7, 1145.
https://doi.org/10.1038/s42003-024-06816-z
Mackey, W. C., & Immerman, R. S. (2001). Restriction of sexual activity as a partial function of disease avoidance: A cultural response to sexually transmitted diseases. Cross-Cultural Research, 35(4), 400-423. https://doi.org/10.1177/106939710103500403
Mackey, W. C., & Immerman, R. S. (2003). New ideas/viewpoints: A proposed feedback loop of sexually transmitted diseases and sexual behavior: The red queen’s dilemma. Social Biology, 50(3-4), 281-299. https://doi.org/10.1080/19485565.2003.9989077
Masliah, E., DeTeresa, R.M., Mallory, M.E., & Hansen, L.A. (2000). Changes in Pathological Findings at Autopsy in AIDS Cases for the Last 15 Years. AIDS, 14 (1), 69-74. https://doi.org/10.1097/00002030-200001070-00008
Mastrorosa, I., Pinnetti, C., Brita, A. C., Mondi, A., Lorenzini, P., Del Duca, G., ... & Antinori, A. (2023). Declining prevalence of human immunodeficiency virus (HIV)–associated neurocognitive disorders in recent years and associated factors in a large cohort of antiretroviral therapy–treated individuals with HIV. Clinical Infectious Diseases, 76(3), e629-e637. https://doi.org/10.1093/cid/ciac658
McArthur, J.C., & Brew, B.J. (2010). HIV-associated Neurocognitive Disorders: Is There a Hidden Epidemic? AIDS, 24(9), 1367-1370. https://doi.org/10.1097/qad.0b013e3283391d56
Meyer-Arndt, L., Kuchling, J., Brasanac, J., Hermann, A., Asseyer, S., Bellmann-Strobl, J., ... & Weygandt, M. (2022). Prefrontal-amygdala emotion regulation and depression in multiple sclerosis. Brain Communications, 4(3), fcac152. https://doi.org/10.1093/braincomms/fcac152
Mohammed, A., Ahmed, M., & Ibrahim, N. (2024). The global seroprevalence of Toxoplasma gondii infection in workers occupationally exposed to animals (1972–2023): a systematic review and meta-analysis. The Veterinary Quarterly, 44(1), 1. https://doi.org/10.1080/01652176.2024.2396577
Pinto, B., Mattei, R., Moscato, G. A., Cristofano, M., Giraldi, M., Scarpato, R., ... & Bruschi, F. (2017). Toxoplasma infection in individuals in central Italy: does a gender-linked risk exist? European Journal of Clinical Microbiology & Infectious Diseases, 36(4), 739-746. https://doi.org/10.1007/s10096-016-2857-8
Pisa, D., Alonso, R., Rábano, A., & Carrasco, L. (2016). Corpora amylacea of brain tissue from neurodegenerative diseases are stained with specific antifungal antibodies. Frontiers in Neuroscience, 10, 86. https://doi.org/10.3389/fnins.2016.00086
Poirotte C., Kappeler P.M., Ngoubangoye B., Bourgeois S., Moussodji M., & Charpentier M.J.E. (2016). Morbid attraction to leopard urine in Toxoplasma-infected chimpanzees. Current Biology, 26, R98–R99. https://doi.org/10.1016/j.cub.2015.12.020
Read A., & Braithwaite V. (2012). Afterword. In: Host Manipulation by Parasites, (eds) D. P. Hughes, J. Brodeur, & F. Thomas (pp. 195-197), Oxford(United Kingdom): Oxford University Press.
Reed, B. D., Zazove, P., Pierson, C. L., Gorenflo, D. W., & Horrocks, J. (2003). Candida transmission and sexual behaviors as risks for a repeat episode of Candida vulvovaginitis. Journal of Women's Health, 12(10), 979-989. https://doi.org/10.1089/154099903322643901
Romero-Pinel, L., Bau, L., Matas, E., León, I., Muñoz-Vendrell, A., Arroyo, P., ... & Martínez-Yélamos, S. (2022). The age at onset of relapsing-remitting multiple sclerosis has increased over the last five decades. Multiple Sclerosis and Related Disorders, 68, 104103. https://doi.org/10.1016/j.msard.2022.104103
Schmid, J., Hunter, P. R., White, G. C., Nand, A. K., & Cannon, R. D. (1995). Physiological traits associated with success of Candida albicans strains as commensal colonizers and pathogens. Journal of Clinical Microbiology, 33(11), 2920-2926. https://doi.org/10.1128/jcm.33.11.2920-2926.1995
Schmid, J., Rotman, M., Reed, B., Pierson, C. L., & Soll, D. R. (1993). Genetic similarity of Candida albicans strains from vaginitis patients and their partners. Journal of clinical microbiology, 31(1), 39-46. https://doi.org/10.1128/jcm.31.1.39-46.1993
Tian, J. Y., Yang, Y. G., Chen, S., Teng, Y., & Li, X. Z. (2021). Genetic diversity and molecular epidemiology of Candida albicans from vulvovaginal candidiasis patients. Infection, Genetics and Evolution, 92, 104893. https://doi.org/10.1016/j.meegid.2021.104893
Tong, W. H., Hlaváčová, J., Abdulai-Saiku, S., Kaňková, Š., Flegr, J., & Vyas, A. (2023). Presence of Toxoplasma gondii tissue cysts in human semen: Toxoplasmosis as a potential sexually transmissible infection. Journal of Infection, 86(1), 60-65. https://doi.org/10.1016/j.jinf.2022.10.034
Tuddenham, S., Koay, W. L., & Sears, C. (2020). HIV, sexual orientation, and gut microbiome interactions. Digestive diseases and sciences, 65(3), 800-817. https://doi.org/10.1007/s10620-020-06110-y
van den Berghe, P. L. (1979). Human Family Systems. An Evolutionary View. New York: Elsevier. https://archive.org/details/humanfamilysyste0000vand
Vyas, A., Kim, S. K., Giacomini, N., Boothroyd, J. C., & Sapolsky, R. M. (2007). Behavioral changes induced by Toxoplasma infection of rodents are highly specific to aversion of cat odors. Proceedings of the National Academy of Sciences, 104(15), 6442-6447. https://doi.org/10.1073/pnas.0608310104
Warszawski, J., Meyer, L., & Bajos, N. (1996). Is genital mycosis associated with HIV risk behaviors among heterosexuals? ACSF Investigators. Analyse des comportements sexuels en France. American Journal of Public Health, 86(8_Pt_1), 1108-1111. https://doi.org/10.2105/AJPH.86.8_Pt_1.1108
Wikipedia. (2025). “HIV/AIDS Public Health Campaigns in Italy” https://en.wikipedia.org/wiki/HIV/AIDS_Public_Health_Campaigns_in_Italy
Wilking, H., Thamm, M., Stark, K. et al. (2016). Prevalence, incidence estimations and risk factors of Toxoplasma gondii infection in Germany: a representative, cross-sectional, serological study. Scientific Reports, 6, 22551. https://doi.org/10.1038/srep22551
Xiao, J., & Yolken, R. H. (2015). Strain hypothesis of Toxoplasma gondii infection on the outcome of human diseases. Acta Physiologica, 213(4), 828. https://doi.org/10.1111/apha.12458
Let me posit a wild theory here: we know t. gondii targets the amygdala; beyond response to immediate danger and lengthening of reaction time, would it be fair to say it could impact our overall perception of danger? And consequently affects us with an attitude where people largely ignore evident threats made to them, even from obviously hostile groups?
Great article.
I'll just add, "You don't know the half of it."
It is transmitted even through dirty hands.
So no one is safe.